One of the most notable features of anorexia nervosa is the intensity and the importance of patients dysfunctional beliefs and values ??related to their weight and shape. The patients’ beliefs and values ??can be seen and understood in cognitive terms.
Anorexia nervosa can be seen as a skill of coping behavior. like all the coping skills, developed from attempts to cope with life events. Poor coping skills developed can include ofgrowing fears and fear of being in their own (separation from parents, a boyfriend, sexuality), feelings of powerlessness, helplessness and worthlessness, and often disturbed or relationships dysfunctional people around the person. The anorexic is concerned with food and weight to distract the self from overwhelming feelings of anxiety, fear and depression, caused by these events. then, the habit of food restriction and ritual so ingrained that the set of behaviors can be separated from its root cause and there by themselves, keeping themselves as functionally autonomous behaviors.
Distorted beliefs, values ??and behaviors or patient’s cognitive distortions are merely symptoms and may assume major importance in the maintenance of the eating disorder. a prerequisite for full recovery is to change these cognitive distortions. For this reason, Christopher Fairburn in 1981 developed a cognitive-behavioral model of treatment for anorexia nervosa and bulimia nervosa. this model uses behavioral interventions and formal cognitive restructuring.
Some of the cognitive distortions that a patient may develop are:
1. I do not need treatment. If I see a therapist or go to a treatment, I will gain weight.
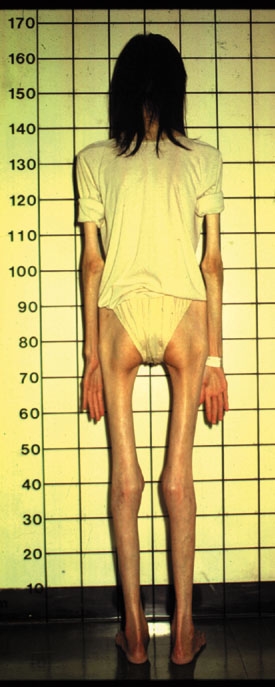
2. I am fat (even though it weighs 90 lbs.)
3. I am not allowed to eat anything until after 9:00 PM. If I do, I will be out of control.
4. Once you start eating normal foods, I will lose control and not being able to stop.
5. If I eat fat, which go right to my thighs.
6. I love wearing tank tops to the mall because people look at me. I know you are just jealous because they look so good.
7. I feel stronger when not eating.
8. I like how I feel when I’m thin.
9. I can keep people away.
10. I am more confident and capable when I’m thin.
Many researchers have drawn on cognitive-behavioral model and proposed their own extensions of the cognitive-behavioral model that integrates cultural and biological influences that may lead to the initiation and maintenance of the habits of anorexics. Proposed that genetic predisposition and nutritional factors were. Affective disorders such as anxiety and depression were prominent etiologic factors, along with family dysfunction and personality variables. Their models include obesity and binge eating. In their model, the weight gain from binge eating leads to the perception of obesity, anorexia and may develop from extreme behaviors for weight control in response to the perception of fat. a prediction of the model is that anorexia is a phobia of weight.
Cognitive-behavioral therapy has been considered the gold standard in the treatment of anorexia. it is still very effective, but the addition of experimental therapies and physiological dramatically increases their effectiveness.